Tuberculosis (TB) remains one of the deadliest infectious diseases in the world, responsible for over a million deaths annually. The fundamental challenge is drug resistance. In Mycobacterium tuberculosis, the bacterium that causes TB, resistance arises through spontaneous chromosomal mutations that allow it to survive exposure to drugs like rifampicin, a cornerstone of first-line TB treatment. The more resistance accumulates, from RR-TB to MDR-TB to XDR-TB, the harder and more toxic the treatment becomes. What makes this especially alarming is that these resistance-causing mutations can go completely undetected. Standard diagnostic tools focus exclusively on mutations within the Rifampicin Resistance-Determining Region (RRDR) of the rpoB gene. But resistance mutations can also arise outside this region, and when they do, current tests return a false “susceptible” result, the wrong treatment is given, and a resistant strain continues to spread silently. It is this critical diagnostic gap that a new review paper by researchers at IIT Guwahati and IIT Madras sets out to address.
Drug resistance in TB arises from chromosomal mutations in Mycobacterium tuberculosis, the bacterium responsible for the disease. These mutations can alter drug targets, block prodrug activation, or overexpress efflux pumps. Of all these mechanisms, drug target modification, particularly hotspot mutations in the rpoB gene, is the most prevalent. Resistance to rifampicin is almost always traced back to mutations within a specific 81-base-pair stretch of this gene, known as the Rifampicin Resistance-Determining Region (RRDR).
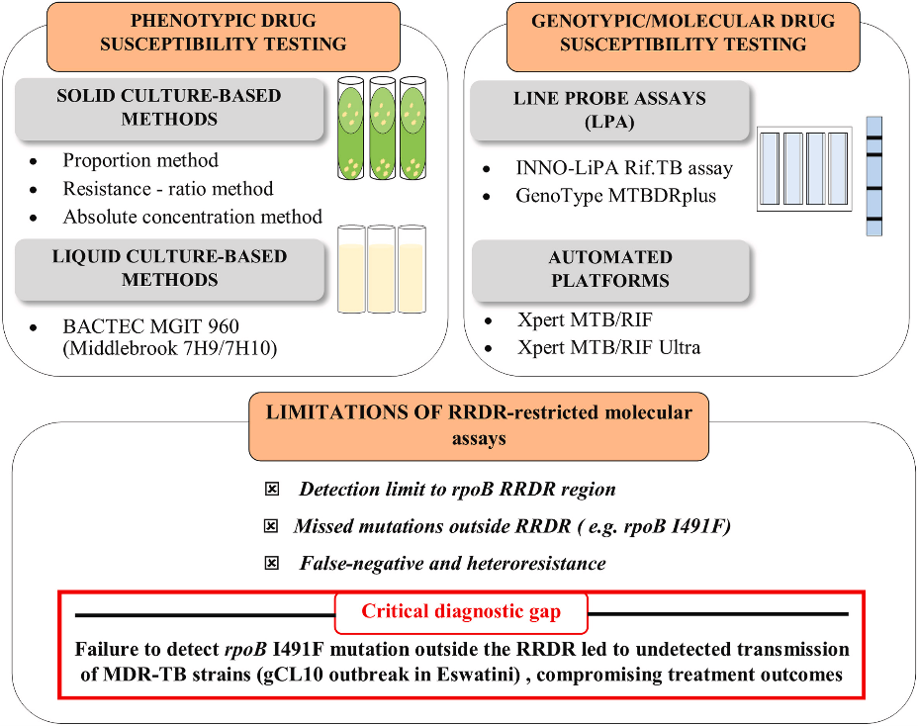
Here lies the problem. Most of the diagnostic tools currently in use, including the widely deployed Xpert MTB/RIF assay and line probe assays, are designed to detect mutations only within the RRDR. But resistance-conferring mutations can also arise outside this region, in what are known as non-RRDR mutations. These mutations are rarer, but they are not negligible, and when present, they are routinely missed by standard diagnostic tests. The consequence? A patient who is actually drug-resistant gets a false “susceptible” result, is put on the wrong treatment, and continues to transmit a resistant strain.
This is precisely the concern that this paper addresses. The authors, Ms. Risha Hazarika from the School of Agro and Rural Technology, IIT Guwahati, and Dr. Sanjukta Patra from the Department of Medical Sciences and Technology, IIT Madras, have comprehensively mapped the molecular basis, epidemiology, and diagnostic blind spots associated with non-RRDR mutations in Mycobacterium tuberculosis.
Two non-RRDR mutations stand out for their clinical significance: I491F and V170F. Both reside near the rifampicin-binding pocket of the RpoB protein and disrupt the drug’s ability to bind effectively. They are not theoretical curiosities, they have been detected in patients across the North Eastern part of India, Myanmar, South Africa, Eswatini, Peru, and beyond, often with very high minimum inhibitory concentrations, meaning the bacteria can survive in the presence of rifampicin concentrations far beyond what is typically used. In Eswatini, for instance, the I491F mutation was found in 30% of MDR-TB isolates tested, yet every single one of them was missed by the standard Xpert MTB/RIF assay. The outbreak strain responsible continued to circulate undetected, and went on to acquire additional resistance.
These mutations can act in two ways. Sometimes, they occur alongside common RRDR mutations, acting as compensatory mutations that offset the fitness cost that drug resistance typically imposes on the bacteria, restoring its growth rate, transmissibility, and virulence. In other cases, they emerge independently, conferring rifampicin resistance all on their own. Either way, the standard tests are blind to them.
The authors review several emerging technologies that can bridge this diagnostic gap. Whole Genome Sequencing (WGS) and Targeted Next-Generation Sequencing (tNGS) are the most comprehensive, capable of detecting the full spectrum of resistance mutations, RRDR and non-RRDR alike. Tools like Deeplex Myc-TB have already demonstrated detection of V170F and I491F mutations from sputum and even stool samples. For settings where sequencing remains expensive and infrastructure-limited, options like Multiplex Allele-Specific PCR (MAS-PCR) and High Resolution Melting Analysis (HRMA) offer faster, lower-cost alternatives that can be deployed in regional laboratories. And on the horizon is nanopore sequencing, a portable, real-time sequencing technology that has already shown the ability to detect non-RRDR mutations and holds promise for decentralised testing.
The bottom line is clear. As long as diagnostic assays are confined to the RRDR region, a significant fraction of drug-resistant TB patients will continue to be misclassified as susceptible, put on ineffective treatment regimens, and serve as silent vectors for the further spread of resistance. For India, which bears one of the highest TB burdens in the world, strengthening the diagnostic toolkit to include non-RRDR mutation detection is not just a scientific priority. It is a public health imperative.

Dr. Luke Elizabeth Hanna, Scientist F & Head, from the Department of Virology & Biotechnology, at ICMR-National Institute for Research in Tuberculosis, gave the following analysis of the work done by the authors of this paper and appreciated their efforts as follows: “This article presents a scholarly review on the evolving genetic landscape of rifampicin resistance in tuberculosis. Rifampicin is one of the most potent first-line drugs used in the treatment of tuberculosis, the number one infectious killer disease that the world is battling to eliminate, and resistance to rifampicin is considered a strong surrogate marker for multidrug-resistant tuberculosis (MDR-TB). This makes the review highly relevant and scientifically important considering the increasing burden of MDR/XDR-TB.
This article is especially valuable because it highlights the diagnostic blind spots in the currently available WHO endorsed molecular tests such as Xpert MTB/RIF, Xpert Ultra and line probe assays that only target mutations present in one small hotspot called the rifampicin resistance determining region (RRDR) of the rpoB gene. The article presents consolidated global evidence on non-canonical resistance-conferring mutations that lie outside the RRDR, and contribute to treatment failure. Inadequate detection of these mutations will also boost emergence of MDR/XDR TB and directly worsen TB control efforts globally. The review also highlights the role of emerging technologies such as whole genome sequencing (WGS), targeted NGS, nanopore sequencing, HRMA and MAS-PCR as promising approaches for detecting both RRDR and non-RRDR mutations.
In brief, this is a well-researched, highly relevant and scientifically important review that seeks to emphasize the point that restricting rifampicin resistance detection to RRDR-association mutations is insufficient and that comprehensive detection of non-RRDR mutations is essential for accurate diagnosis, effective treatment and improved global control of drug-resistant tuberculosis.”
Article by Akshay Anantharaman
Click here for the original link to the paper